Free Har 3 Connecticut PDF Template
Free Har 3 Connecticut PDF Template
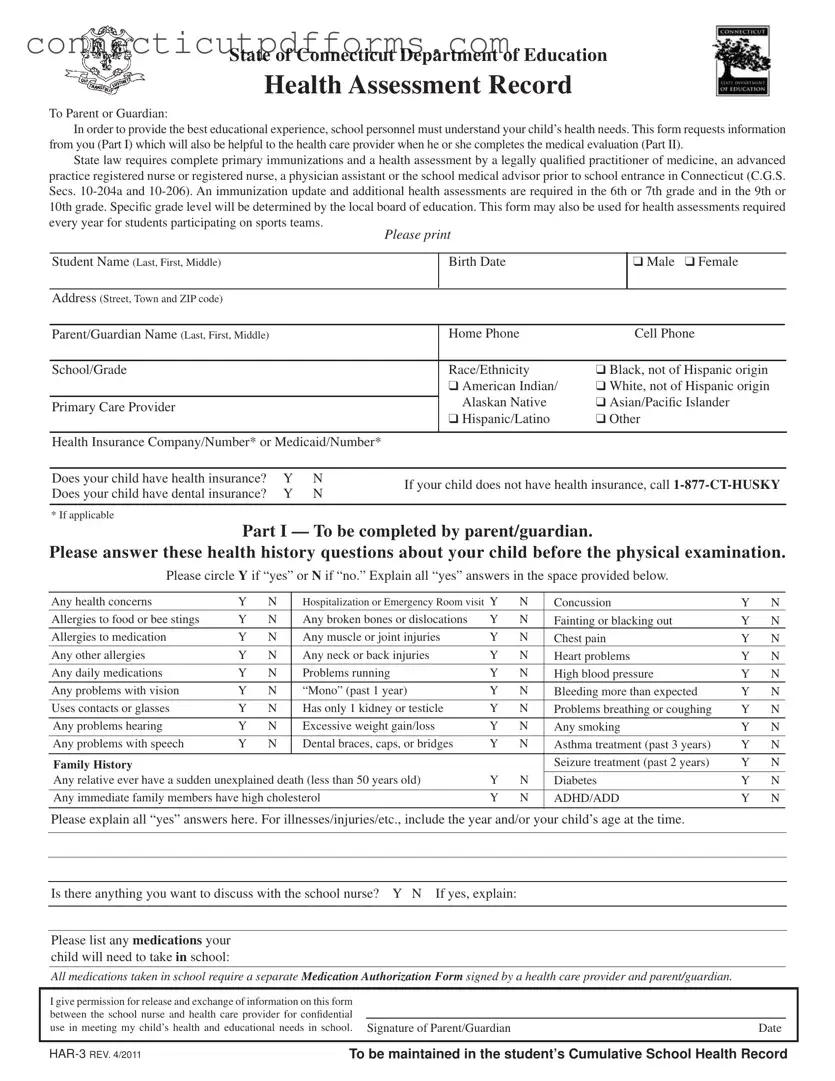
The HAR 3 Connecticut form is an essential tool for ensuring that students receive the necessary health assessments before entering school. This form serves multiple purposes, beginning with the collection of vital health information from parents or guardians in Part I. It captures details about the child's medical history, including immunizations, allergies, and any existing health concerns. This information is crucial not only for school personnel but also for health care providers who will conduct the medical evaluations in Part II. Connecticut law mandates that students must have complete primary immunizations and a health assessment conducted by qualified medical professionals before they can attend school. The form also outlines the need for updates on immunizations and health assessments at specific grade levels, such as 6th or 7th grade and 9th or 10th grade, as determined by local education authorities. Furthermore, it accommodates students participating in sports by requiring annual health assessments. Parents will find sections to indicate their child's health insurance status and any medications needed during school hours. The thoroughness of this form aims to create a safe and supportive educational environment, addressing the health needs of each student effectively.
Connecticut Sba 2 - Ensure you provide accurate information as you wish it to appear in the Board's records.
To ensure a smooth rental experience, it is beneficial for landlords and tenants to familiarize themselves with the specifics of the New York Lease Agreement form. This document is crucial for clearly defining the relationship and obligations between the parties involved. For those seeking additional insights or templates, Templates and Guide can provide valuable resources to navigate this process effectively.
Connecticut Op 300 - Reporting periods must be specified at the top of the OP-300 form.
Ct Dmv Registration Requirements - Filing this form allows military members to avoid unnecessary financial burdens while serving the country.
| Fact Name | Description |
|---|---|
| Purpose | The HAR-3 form is used to collect health information from parents or guardians to ensure schools understand a child's health needs. |
| Governing Laws | This form is governed by Connecticut General Statutes Sections 10-204a and 10-206, which mandate health assessments and immunizations for school entrance. |
| Immunization Requirements | Complete primary immunizations are required before school entry. Additional updates are needed in the 6th or 7th grade and in the 9th or 10th grade. |
| Health History | Part I of the form requires parents to answer health history questions, which help healthcare providers during evaluations. |
| Annual Assessments | The form can also be used for annual health assessments for students participating in sports teams. |
| Signature Requirement | A signature from the parent or guardian is required to authorize the release of health information between the school and healthcare providers. |
| Medical Evaluation | Part II must be completed by a healthcare provider, including a physical examination and assessment of health history. |
| Insurance Information | The form collects information regarding the child’s health and dental insurance status, which is vital for accessing healthcare services. |
State of Connecticut Department of Education
Health Assessment Record
To Parent or Guardian:
In order to provide the best educational experience, school personnel must understand your child’s health needs. This form requests information from you (Part I) which will also be helpful to the health care provider when he or she completes the medical evaluation (Part II).
State law requires complete primary immunizations and a health assessment by a legally qualiied practitioner of medicine, an advanced
practice registered nurse or registered nurse, a physician assistant or the school medical advisor prior to school entrance in Connecticut (C.G.S.
Secs.
every year for students participating on sports teams.
Please print
Student Name (Last, First, Middle) |
Birth Date |
|
❑ Male ❑ Female |
|
|
|
|
|
|
Address (Street, Town and ZIP code) |
|
|
|
|
|
|
|
|
|
Parent/Guardian Name (Last, First, Middle) |
Home Phone |
|
Cell Phone |
|
|
|
|
||
School/Grade |
Race/Ethnicity |
❑ Black, not of Hispanic origin |
||
|
❑ American Indian/ |
❑ White, not of Hispanic origin |
||
|
Alaskan Native |
❑ Asian/Paciic Islander |
||
Primary Care Provider |
||||
|
❑ Hispanic/Latino |
❑ Other |
||
|
|
|
|
|
Health Insurance Company/Number* or Medicaid/Number*
Does your child have health insurance? |
Y |
N |
If your child does not have health insurance, call |
|
Does your child have dental insurance? |
Y |
N |
||
|
||||
|
|
|
|
|
* If applicable |
|
|
|
Part I — To be completed by parent/guardian.
Please answer these health history questions about your child before the physical examination.
Please circle Y if “yes” or N if “no.” Explain all “yes” answers in the space provided below.
Any health concerns |
Y |
N |
Hospitalization or Emergency Room visit Y |
N |
Concussion |
Y |
N |
|
Allergies to food or bee stings |
Y |
N |
Any broken bones or dislocations |
Y |
N |
Fainting or blacking out |
Y |
N |
Allergies to medication |
Y |
N |
Any muscle or joint injuries |
Y |
N |
Chest pain |
Y |
N |
Any other allergies |
Y |
N |
Any neck or back injuries |
Y |
N |
Heart problems |
Y |
N |
Any daily medications |
Y |
N |
Problems running |
Y |
N |
High blood pressure |
Y |
N |
Any problems with vision |
Y |
N |
“Mono” (past 1 year) |
Y |
N |
Bleeding more than expected |
Y |
N |
Uses contacts or glasses |
Y |
N |
Has only 1 kidney or testicle |
Y |
N |
Problems breathing or coughing |
Y |
N |
|
|
|
|
|
|
|
|
|
Any problems hearing |
Y |
N |
Excessive weight gain/loss |
Y |
N |
Any smoking |
Y |
N |
Any problems with speech |
Y |
N |
Dental braces, caps, or bridges |
Y |
N |
Asthma treatment (past 3 years) |
Y |
N |
|
|
|
|
|
|
|
|
|
Family History |
|
|
|
|
|
Seizure treatment (past 2 years) |
Y |
N |
Any relative ever have a sudden unexplained death (less than 50 years old) |
Y |
N |
Diabetes |
Y |
N |
|||
|
|
|
|
|
|
|||
Any immediate family members have high cholesterol |
Y |
N |
ADHD/ADD |
Y |
N |
|||
|
|
|
|
|
|
|
|
|
Please explain all “yes” answers here. For illnesses/injuries/etc., include the year and/or your child’s age at the time.
Is there anything you want to discuss with the school nurse? Y N If yes, explain:
Please list any medications your child will need to take in school:
All medications taken in school require a separate Medication Authorization Form signed by a health care provider and parent/guardian.
I give permission for release and exchange of information on this form between the school nurse and health care provider for conidential
use in meeting my child’s health and educational needs in school. Signature of Parent/Guardian |
Date |
|
|
|
|
TO BE MAINTAINED IN THE STUDENT’S CUMULATIVE SCHOOL HEALTH RECORD |
||
Part II — Medical Evaluation
Health Care Provider must complete and sign the medical evaluation and physical examination
Student Name |
|
Birth Date |
|
Date of Exam |
❑I have reviewed the health history information provided in Part I of this form
Physical Exam
Note: *Mandated Screening/Test to be completed by provider under Connecticut State Law
*Height _____ in. / _____% *Weight _____ lbs. / _____% |
BMI _____ / _____% Pulse _____ |
*Blood Pressure _____ / _____ |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Normal |
|
Describe Abnormal |
|
|
Ortho |
|
|
Normal |
|
Describe Abnormal |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Neurologic |
|
|
|
|
|
|
Neck |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HEENT |
|
|
|
|
|
|
Shoulders |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
*Gross Dental |
|
|
|
|
|
|
Arms/Hands |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Lymphatic |
|
|
|
|
|
|
Hips |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Heart |
|
|
|
|
|
|
Knees |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Lungs |
|
|
|
|
|
|
Feet/Ankles |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Abdomen |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
*Postural |
❑ No spinal |
❑ Spine abnormality: |
|||||||||
|
|
|
|
|
|
|
|
||||||||||
Genitalia/ hernia |
|
|
|
|
|
|
|
|
abnormality |
|
❑ Mild |
❑ Moderate |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❑ Marked ❑ Referral made |
|||
Skin |
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Screenings |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
*Vision Screening |
|
|
|
*Auditory Screening |
|
|
|
|
|
|
|
Date |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Type: |
Right |
Left |
|
Type: |
Right |
Left |
|
|
Lead: |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
❑ Pass |
❑ Pass |
|
|
|
|
|
|
||||
|
With glasses |
20/ |
20/ |
|
|
|
|
*HCT/HGB: |
|
|
|
||||||
|
|
|
|
|
|
|
❑ Fail |
❑ Fail |
|
|
|
|
|
|
|
|
|
|
Without glasses |
20/ |
20/ |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
*Speech (school entry only) |
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
||||||||
|
❑ Referral made |
|
|
|
❑ Referral made |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
Other: |
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
TB: |
❑ No |
❑ Yes |
|
PPD date read: |
|
|
Results: |
|
|
|
Treatment: |
|
|
|
||
*IMMUNIZATIONS
❑Up to Date or ❑
*Chronic Disease Assessment:
Asthma |
❑ No |
❑ Yes: |
❑ Intermittent ❑ Mild Persistent ❑ Moderate Persistent ❑ Severe Persistent ❑ Exercise induced |
||||
|
If yes, please provide a copy of the Asthma Action Plan to School |
|
|||||
Anaphylaxis ❑ No |
❑ Yes: |
❑ Food |
❑ Insects |
❑ Latex |
❑ Unknown source |
|
|
Allergies |
If yes, please provide a copy of the Emergency Allergy Plan to School |
|
|||||
|
History of Anaphylaxis |
❑ No |
❑ Yes |
Epi Pen required ❑ No |
❑ Yes |
||
Diabetes |
❑ No |
❑ Yes: |
❑ Type I |
❑ Type II |
Other Chronic Disease: |
|
|
Seizures |
❑ No |
❑ Yes, type: |
|
|
|
|
|
❑This student has a developmental, emotional, behavioral or psychiatric condition that may affect his or her educational experience. Explain: ____________________________________________________________________________________________________
Daily Medications (specify): ____________________________________________________________________________________
This student may: ❑ participate fully in the school program
❑participate in the school program with the following restriction/adaptation: _____________________________
___________________________________________________________________________________________________________
This student may: ❑ participate fully in athletic activities and competitive sports
❑participate in athletic activities and competitive sports with the following restriction/adaptation: ____________
___________________________________________________________________________________________________________
❑Yes ❑ No Based on this comprehensive health history and physical examination, this student has maintained his/her level of wellness.
Is this the student’s medical home? ❑ Yes ❑ No ❑ I would like to discuss information in this report with the school nurse.
|
|
|
|
|
|
Signature of health care provider MD / DO / APRN / PA |
Date Signed |
Printed/Stamped Provider Name and Phone Number |
|
|
|
|
|
|
Student Name: ______________________________________ Birth Date: ___________________
Immunization Record
To the Health Care Provider: Please complete and initial below.
Vaccine (Month/Day/Year) Note: *Minimum requirements prior to school enrollment. At subsequent exams, note booster shots only.
|
Dose 1 |
Dose 2 |
|
Dose 3 |
|
Dose 4 |
|
Dose 5 |
|
Dose 6 |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
DTP/DTaP |
* |
* |
|
* |
|
* |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DT/Td |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Tdap |
* |
|
|
|
|
|
|
Required for 7th grade entry |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
IPV/OPV |
* |
* |
|
* |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MMR |
* |
* |
|
|
|
|
|
Required |
||||
|
|
|
|
|
|
|
|
|
|
|
||
Measles |
* |
* |
|
|
|
|
|
Required |
||||
|
|
|
|
|
|
|
|
|
|
|
||
Mumps |
* |
* |
|
|
|
|
|
Required |
||||
|
|
|
|
|
|
|
|
|
|
|
||
Rubella |
* |
* |
|
|
|
|
|
Required |
||||
|
|
|
|
|
|
|
|
|
|
|
||
HIB |
* |
|
|
|
|
|
|
PK and K (Students under age 5) |
||||
|
|
|
|
|
|
|
|
|
|
|
||
Hep A |
* |
* |
|
|
|
|
|
PK and K (born 1/1/2007 or later) |
||||
|
|
|
|
|
|
|
|
|
|
|
||
Hep B |
* |
* |
|
* |
|
|
|
Required |
||||
|
|
|
|
|
|
|
|
|
|
|
||
Varicella |
* |
* |
|
|
|
|
|
2 doses required for K & 7th grade as of 8/1/2011 |
|
|||
|
|
|
|
|
|
|
|
|
|
|
||
PCV |
* |
|
|
|
|
|
|
PK and K (born 1/1/2007 or later) |
||||
|
|
|
|
|
|
|
|
|
|
|
||
Meningococcal |
* |
|
|
|
|
|
|
Required for 7th grade entry |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
HPV |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Flu |
* |
|
|
|
|
|
|
PK students |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Disease Hx ________________________________ |
________________________________ |
________________________________ |
|
|
||||||||
of above |
(Specify) |
|
|
(Date) |
|
|
|
(Conirmed by) |
|
|
|
|
|
|
|
|
Exemption |
|
|
|
|
|
|
|
|
|
Religious _____ Medical: Permanent _____ |
Temporary _____ Date _____ |
|
|
|
|||||||
|
Recertify Date _________ |
Recertify Date _________ Recertify Date ________ |
|
|
|
|||||||
Immunization Requirements for Newly Enrolled Students at Connecticut Schools
KINDERGARTEN
•DTaP: At least 4 doses. The last dose must be given on or after 4th birthday.
•Polio: At least 3 doses. The last dose must be given on or after 4th birthday.
•MMR: 2 doses given at least 28 day apart – 1st dose on or after the 1st birthday.
•Hib: 1 dose on or after 1st birthday (Children 5 years and older do not need proof of Hib vaccination).
•Pneumococcal: 1 dose on or after 1st birthday (born 1/1/2007 or later and less than 5 years old).
•Hep A: 2 doses given six months
•Hep B: 3
•Varicella: For students enrolled before August 1, 2011, 1 dose given on or after 1st birthday; for students enrolled on or after August 1, 2011
2 doses given 3 months apart – 1st dose on or after 1st birthday or veriication of disease*.
GRADES
•DTaP /Td/Tdap: At least 4 doses. The last dose must be given on or after 4th birthday;
students who start the series at age 7 or older only need a total of 3 doses of
•Polio: At least 3 doses. The last dose must be given on or after 4th birthday.
•MMR: 2 doses given at least 28 days apart- 1st dose on or after the 1st birthday.
•Hep B: 3 doses – the last dose on or after 24 weeks of age.
•Varicella: 1 dose on or after the 1st birthday or veriication of disease*.
GRADE 7
•Tdap/Td: 1 dose of Tdap for students 11 yrs. or older enrolled in 7th grade who completed their primary DTaP series; For those students who start the series at age 7 or older a total of 3 doses of
•Polio: At least 3 doses. The last dose must be given on or after 4th birthday.
•MMR: 2 doses given at least 28 days apart – 1st dose on or after the 1st birthday.
•Meningococcal: one dose for students enrolled in 7th grade.
•Hep B: 3
•Varicella: 2 doses given 3 months apart – 1st dose on or after 1st birthday or veriication of
disease*.
GRADES
•Td: At least 3 doses. Students who start the series at age 7 or older only need a total of 3 doses of
•Polio: At least 3 doses. The last dose must be given on or after 4th birthday.
•MMR: 2 doses given at least 28 days apart- 1st dose on or after the 1st birthday.
•Hep B: 3
•Varicella: For students <13 years of age, 1 dose given on or after the 1st birthday. For
students 13 years of age or older, 2 doses given at least 4 weeks apart or veriication of
disease*.
*Veriicationofdisease:Conirmation in writ- ing by a MD, PA, or APRN that the child has a previous history of disease, based on family or medical history.
|
|
|
|
|
|
Initial/Signature of health care provider MD / DO / APRN / PA |
Date Signed |
Printed/Stamped Provider Name and Phone Number |
|
|
|
|
|
|
Filling out the HAR 3 Connecticut form can be a straightforward process, but several common mistakes can lead to delays or complications. One frequent error is neglecting to provide complete information in the student’s personal details section. This includes the full name, birth date, and address. Missing or incorrect details can hinder communication between the school and healthcare providers.
Another common mistake is failing to answer the health history questions thoroughly. Parents or guardians should circle "Y" for yes or "N" for no for each question. Omitting answers or leaving questions blank can result in critical health information being overlooked. It is essential to explain any "yes" responses in the designated space, as this information helps school staff understand the child's health needs better.
Some individuals mistakenly believe that the health assessment form is optional. In reality, Connecticut law mandates that a complete health assessment be submitted before a child enters school. This includes immunization records and a medical evaluation by a qualified healthcare provider. Parents should ensure that these documents are attached to the HAR 3 form.
Another error involves misunderstanding the immunization requirements. Parents must provide accurate vaccination history, including dates and types of vaccines received. Failing to include this information can lead to the child being unable to attend school until the records are complete. Always check that the immunization record is up to date and attached.
In some cases, parents overlook the need to indicate whether their child has health insurance. This information is crucial for the school to assist families in accessing healthcare services. If a child does not have insurance, it is important to follow up with the appropriate resources, such as the HUSKY program.
Furthermore, many parents forget to sign the form. A signature is necessary to authorize the release of information between the school and healthcare provider. Without it, the form may be considered incomplete, delaying the processing of health records.
Another mistake is not discussing specific health concerns with the school nurse. If there are issues that may affect the child’s educational experience, it’s vital to communicate those needs clearly. This dialogue can help ensure that the school is prepared to support the child effectively.
Additionally, parents sometimes fail to provide a list of medications that their child will need to take during school hours. This omission can lead to misunderstandings about a child's medication needs, which can impact their health and well-being while at school. It is crucial to list all medications and ensure that a separate Medication Authorization Form is completed.
Lastly, parents may not keep copies of the completed HAR 3 form for their records. Retaining a copy ensures that parents have access to the information provided and can reference it in future health assessments or discussions with school personnel. Keeping organized records can save time and effort in the long run.
Filling out the HAR 3 Connecticut form is an important step in ensuring that your child receives the best possible educational experience. Here are some key takeaways to keep in mind:
Completing the HAR 3 form accurately and thoroughly helps create a supportive environment for your child in school. It not only fulfills legal requirements but also contributes to their overall well-being.
The HAR-3 Connecticut form shares similarities with the Child Health Assessment form, commonly used in various states. Both documents require parents or guardians to provide comprehensive health information about their children, including medical history and any current health issues. Like the HAR-3, the Child Health Assessment form is designed to facilitate communication between parents and healthcare providers, ensuring that the child’s health needs are met as they enter school or participate in activities.
Another document akin to the HAR-3 is the Sports Physical Form. This form is specifically tailored for students participating in athletics and requires a medical evaluation to ensure that the child is fit for physical activity. Similar to the HAR-3, it collects health history, assesses any pre-existing conditions, and requires a healthcare provider's signature. Both forms aim to safeguard the health of students while participating in school-related activities.
The Immunization Record is another related document. This record tracks a child's vaccination history and is crucial for school enrollment, much like the immunization section of the HAR-3. Both documents ensure that students meet state requirements for vaccinations before attending school, thus protecting public health and preventing outbreaks of communicable diseases.
The School Health Record serves a similar purpose to the HAR-3 by maintaining an ongoing record of a student’s health assessments and immunizations throughout their educational journey. Both documents are kept confidential and are vital for school nurses to monitor and address the health needs of students effectively.
If you're looking to streamline your asset transactions, understanding the various forms available is essential. One such important document is the comprehensive bill of sale for personal property. For more information, you can explore our guide on the bill of sale process.
Additionally, the Health History Questionnaire is comparable to the HAR-3. This form gathers detailed information about a child's past medical history, allergies, and medications. Parents fill out both forms to provide essential health information that informs healthcare providers about the child's needs, ensuring appropriate care is given in school settings.
The Medication Authorization Form is another document that aligns with the HAR-3. This form is necessary when a child requires medication during school hours. Both documents require signatures from parents and healthcare providers, emphasizing the importance of proper medication management and communication between parents and school officials.
The Individualized Education Program (IEP) often includes health-related information and is similar to the HAR-3 in its focus on a child's specific needs. While the HAR-3 addresses general health assessments, the IEP provides a tailored plan for students with disabilities, ensuring that their health needs are integrated into their educational goals.
The 504 Plan is also comparable to the HAR-3 as it outlines accommodations for students with disabilities. Like the HAR-3, it addresses health-related issues that may impact a student's ability to succeed in school. Both documents are designed to ensure that all students receive the support they need to thrive in an educational environment.
Lastly, the Family Health History form is similar to the HAR-3 in that it collects information about health conditions that may run in a family. This information is crucial for understanding potential health risks and is often a part of the health assessment process for school-aged children. Both forms aim to create a comprehensive picture of a child's health to better inform their care and educational experience.